Originally published at Forbes.com on September 2, 2022.
The headline of Wednesday’s New York Times report announces, “U.S. Life Expectancy Falls Again in ‘Historic’ Setback,” and the just-released data from the CDC is shocking: During the second year of the pandemic, life expectancy not only didn’t recover from its 2020 drop, but it dropped further, from 78.8 years in 2019 to 77 in 2020, down further to 76.1 years in 2021, based on provisional data.
What’s more, gaps among ethnic/racial groups (mostly) widened sharply.
To be sure, Hispanic and Asian-ethnicity Americans’ life expectancy remained higher than that of (non-Hispanic) white Americans, in line with general patterns in which immigrants have greater life expectancy than native born residents, though the gap for Hispanics narrowed, from 3.1 years’ greater life expectancy to only 1.3 years. (For Asian-ethnicity Americans, the gap widened slightly, from 6.8 to 7.1 years.)
However, for Black Americans, the 4 year lower life expectancy in 2019 became 5.6 years in 2021. And for American Indian/Alaskan Natives (AIAN, in CDC parlance), the drop was even worse, from a 7 year gap at 71.8 years to an 11.2 year gap at 65.2 years’ life expectancy.
To what extent, are these drops of life expectancy due to Covid-19, rather than other causes?
From 2019 to 2020, the CDC reports that 90% of the drop in Hispanic life expectancy was attributable to Covid; the corresponding rates were 68% for whites and 59% for blacks. (No breakdown was provided for the AIAN or Asian categories.) However, the CDC data splits its breakdowns into “contributions to decreases” and “contributions to increases” rather than overall net effect. Those readers who are used to looking at data and charts will expect a “waterfall” style chart; the CDC version is not this, and is not particularly helpful.
In any event, relative to the 2020 baseline, the further decreases in life expectancy during 2021 had multiple causes. Only among the White demographic group was Covid the cause of over half of the decline; unintentional injury (including overdoses) was the second-largest contributing factor and for the AIAN demographic group, worsening rates of death due to chronic liver disease and cirrhosis played almost as substantial a role.
And, finally, it is important to understand that the CDC data shows a continued improvement in life expectancy due to reductions in death due to such causes as influenza/pneumonia, COPD/emphysema, Alzheimer disease, diabetes, and perinatal conditions (infant deaths). In fact, strikingly, in 2021, heart disease was a contributor to increased life expectancy in the Black, Hispanic, and Asian demographic groups, but a contributor to decreased life expectancy for the White and AIAN groups.
Again, though, the way the CDC provides its information means that, when it comes down to it, there is much that is simply missing; we do not know the magnitude of the improvements in life expectancy due to these causes, just that it exists. It even seems likely, or at least possible, that some of the apparent improvement in mortality due to these factors was actually because deaths were actually recorded as Covid deaths instead (whether due to multiple causes of death or other reasons).
Having said all this, it is important to understand what “life expectancy” means in the first place. Yes, these rates dropped in 2020 and 2021 — but that does not mean that you, or I, have had our own personal life expectancy shortened.
The type of life expectancy calculation reported by the CDC is called “period life expectancy.” As life insurance actuary Mary Pat Campbell explains, period life expectancy takes “the mortality experience for the whole population during a specific time period, usually a single year (in this case, 2021), and then calculat[es] life expectancy as if the mortality seen by the full population during that year was the one a person would be seeing during a lifetime. No person actually lives through a mortality pattern like this, because we’re not in a ‘steady state’ for mortality.”
Do we expect the Covid death rates we saw in 2020 or 2021 to continue indefinitely? If not, then period life expectancy is not a helpful measure for planning for the future, and actuaries, demographers, and others turn to cohort life expectancy based on specific birth years, for example, how many more remaining years of life someone born in 1970 can be expected to have, on average.
Period life expectancy is not useless, of course; it’s a snapshot, and a simple yardstick for measuring the overall health and well-being of a country or a demographic group from one time period to the next. But as we saw in trying to unpack the specific causes of deaths that play into this, period life expectancy is too simple a figure to give us a real understanding of covid impacts or other trends.
Instead, as again, Mary Pat Campbell explains, what’s really much more useful to provide this broader understanding is the mortality rate, which can be unpacked by age group, to see the impact of Covid and other causes of death: for young adults, up through age 35, there was more excess (above-average) mortality due to drug overdoses during the pandemic years, than due to covid; for Gen Xers, as they go from their early 40s to their late 50s, covid shifts from the highest-ranking among multiple causes of excess mortality to the cause which far overshadows all others; and the dominance of Covid in the causes of excess mortality only increases for Boomers and the Silent generation, where Campbell explains discusses the life expectancy improvement factors in the CDC data:
“There are a few possibilities here, given the delta/omicron wave of 2021. First, we have the ‘they would have died of something anyway’ explanation — that explains why someone who would have died of heart disease died of COVID instead in 2021. Remember, total mortality for the age 85+ group was still higher in 2021 than in 2019. It’s just that a bunch of causes of death were also lower than usual, unlike what we saw with other adult age groups.
“But let’s think of that increase in Alzheimer’s deaths in 2020 — could be the nursing home deaths of 2020, could be due to neglect during lockdowns and other causes. This could be a ‘they died earlier, so they couldn’t die later’ explanation.”
Campbell’s data also provides visualizations of the degree to which mortality rate-improving factors had an effect — turns out the magnitude of these offsetting factors is actually very small, except for in the oldest-old.
Now, this sort of analysis of mortality data is far more enlightening than the data that the CDC provides, and it would be great to see Campbell’s graphs split out by racial/ethnic group to better understand that dramatic headline statistics reported by the Times and elsewhere, but, honestly, Campbell isn’t being paid by anyone to produce this data and it would be nice for the people who are being paid to produce something as helpful as her tables and charts.
Author’s note: the terms of my affiliation with Forbes enable me to republish materials on other sites, so I am updating my personal website by duplicating a selected portion of my Forbes writing here.
Do we now have conclusive proof that masking works? No. Do we have data that strongly suggests this to be the case? Yes. Is it all wrapped up in questions of how to interpret such studies, and the inherent difficulty of studies that can only attempt to approximate an experiment rather than truly being one? Also yes.
Here’s the background: a group of researchers and aid workers from Poverty Action, funded by the charity Give Well, undertook a massive study in Bangladesh to test mask-wearing — but you can’t simply force one group of people to wear masks and prohibit another group, particularly at the village-by-village level, so what they undertook were a series of actions designed to promote mask-wearing.
To begin with, they designated certain villages “control” and others “treatment” in the same way as, with a test of a medication, a certain group would get the placebo and others, the real medicine. The control villages received, nothing, but the “treatment” village, through a process of randomization, either were given cloth masks or surgical masks, for the duration of a 10-week period, and, with further randomization, were given further inducements to wear masks, such as encouragement from imams and other “village elders,” or texts from experts encouraging mask-wearing as an altruistic action or for one’s own benefit, or other such encouragements. They then measured the degree to which these inducements resulted in more mask-wearing, by having observers count the number of people wearing masks in public places, and found that they were able to triple the rate at which people wore their masks in public.
Now, to be clear, the entire “package” was implemented for the main test group: free mask distribution alongside encouragement to wear the masks and role-modeling by public officials and community leaders, which included a video with the head imam and a national cricket star shown when the masks were distributed, as well as promotion by local imams during Friday prayers using a scripted speech and further unspecified “mask promotion in public spaces.” Some villages also received monetary or non-monetary incentives for village-wide compliance, a program of asking households to commit to mask-wearing with a pledge and a front-door sign, and a set of text messages; and villages were also randomly assigned to receive either cloth or surgical masks. After 8 weeks, they stopped the “intervention” but kept tallying mask-wearing for a further two weeks.
The result was that mask-wearing in the treatment villages increased by 29 percentage points or, using a different method of analysis, 28.1 points, relative to a baseline of 13.3%. Surprisingly, the additional boosting efforts had no effect: none of the by-village monetary incentive, text-encouragement, or public front-door sign program made a difference – in fact, these most likely reduced levels of mask-wearing. The only factors that were associated with greater rates of mask-wearing were being given a surgical (rather than cloth) mask and being given a mask that was blue rather than green or purple rather than red.
(Yes, really – the effect on mask-wearing of having a purple cloth mask was quite substantial. The mask colors were used to identify people who had received different sorts of “private” nagging in terms of the text messages, but the meaning of the color used was varied between village. Green symbolizes Islam; was this color seen as sacrilegious? Was there a different, negative connotation to red, or positive connotation to purple? This unexpected difference is a bit disconcerting, because it suggests that the researchers did not have the understanding of local culture that they should have to conduct research, even if there’s nothing else fishy about it.)
But this was only the first step in their study. Their larger objective was to measure the degree to which the free-mask/mask-encouragement-induced greater mask-wearing reduced covid cases – and, indeed, they find substantially lower rates for the treatment than the control groups, based on testing everyone who reports covid symptoms during the study period. (Two complications here: first, they only tested those who reported symptoms, and only about 40% of those reporting symptoms agreed to be tested.)
The results here are fairly dramatic, or are so at first glance, at least: relative to the control villages, those villages given surgical masks had an 11% reduction in (symptomatic) covid prevalence over the 10 week period. For those above 60, those at highest risk, the results are even more dramatic, a decrease in infection of 35%. Considering that, even with these interventions, fewer than 50% of people observed wore masks, this suggests that consistent mask-wearing by everyone would have an even greater effect. And, in fact, the authors do the math of how much it cost them to provide the masks, the mask-promotion, and the mask-wearer counting, to conclude that it is entirely feasible, in terms of lives saved, to expand these efforts.
The study also looked at the impact of mask-wearing on physical distancing – not so much because it was their goal to push Bangladeshis into more distancing but because one theory was that mask-wearing would, due to risk-compensation, result in people distancing less. Instead, within mosques, people distanced as much as before, but in other circumstances, distancing increased.
But the study left a number of questions unanswered – or, at least, I didn’t see the answers.
We know that treatment villages were given masks and non-treatment villages were not – but the latter villages were still surveyed by phone and asked about symptoms, then those reporting covid symptoms were asked to test, which about 40% consented to. The study did not indicate what percent of villagers responded to the survey, or how they perceived the study, or whether they resented being called and asked questions when only the neighboring village, not they themselves, received masks.
The study also did not report on any issues of variation within the treatment villages, except to the extent that standard errors are reported for mask-wearing (and, honestly, I’m not good enough at the stats part to get a sense of interpretation here). Was there an (inverse) correlation between village-wide mask-wearing and covid prevalence? That would make the relationship between masks and covid-reduction clearer. Is there a reason why this statistical calculation/test would be invalid? The villages are all also presented as simply generic “one no different than the next” villages, and maybe that’s indeed true, or the randomization process makes differences irrelevant, but I would imagine that there are still real differences, whether they be a matter of some regions of the country being richer or poor than others, or having different age pyramids (different fertility rates, different rates of out-migration to the city).
Also, all observations were conducted outside except for mosques, because there simply weren’t non-mosque indoor spaces. But it is generally not considered particularly risky to wear masks outdoors, and the paper doesn’t state whether villagers were told to wear masks any time they were outside their own homes, or what instructions in particular they were given regarding times and circumstances in which it was necessary to wear a mask, and when the risk was low enough not to. Or is Bangladeshi public/outdoor life as crowded as indoor American life?
Another surprising element is the two pilot studies that informed their ultimate large-scale study. In the first study, they had free masks and an educational campaign, and boosted mask-wearing rates by 10.9 percentage points. In the second pilot, they added the presence of workers whose role was to “remind” villagers to wear their mask, and they boosted the rate to a level matched in the final study, 28.4 percentage points. Honestly, I have trouble making sense of this – isn’t a village in Bangladesh exactly the sort of place where outsiders would be very visibly “outside” and not able to persuade much? Or were “locals” hired in this role? This seems to be another “cultural” issue. As it happens, one of the criticisms of the study is that symptoms were self-reported rather than based on objective testing, so that if the villagers in test villages believed that there was a particular reason to minimize symptoms (to prove they were compliant, to avoid dishonoring the village, to show loyalty to village elders, etc.), this would cause problems with the study, and their surprising degree of responsiveness to individual “persuaders” suggests to me that this is possible.
Another issue is the differentiation between surgical and cloth masks. The key data element is, again, that control villages had a prevalence of covid of 0.76% cloth mask villages had a prevalence of .74%, and surgical mask villages, .67%. There was therefore no statistically-significant effect from cloth masks – which of course should raise concerns for places such as the US where “even a bandana will do” has been the operative approach. But in any case, there was a higher rate of mask-wearing for surgical mask villages, even though the difference wasn’t statistically-significant. It does nonetheless raise the question of whether the surgical mask was what made the difference, or the greater likelihood of mask-wearing in surgical-mask villages.
Another issue: age group differences. For surgical mask villages only, they split out covid rates by age. For those younger than age 50, there was no difference in covid infections between this villages and the control villages. For those 50 – 60 years old, there was a decrease of 23%. For those over age 60, there was a decrease of 35%. What would account for this difference? The study does not identify different mask-wearing rates for different ages (presumably they did not attempt to guess the age of the mask-wearers or non-mask-wearers they saw), and, in theory, this shouldn’t matter, as the theory of mask-wearing is that it protects others, so that the entire community should see declines. However, the study (to prove risk compensation was not happening) showed that there were greater degrees of physical distancing in treatment villages. Did the project of mask-wearing result in overall greater degrees of caution, especially among older Bangladeshis?
This is a point of contention among critics, as well as the general element of the increased physical distancing. If physical distancing could be the cause of reduced spread, or if other elements explain the reduction only among the old, then did the intervention “work”? Or, rather, what does it mean to say the intervention “worked” if it was plausibly the knock-on effects of mask-wearing and what we want to demonstrate is that masking can substitute for undesirable alternate interventions like distancing or lockdowns?
Here are some other criticisms I’m seeing.
First, from an anonymous commenter on twitter: the difference between cloth and surgical mask-wearing isn’t statistically significant when measured with something called an “intervention prevalence ratio,” which is more-or-less the difference in rates provided above. On this basis, a confidence interval for either cloth or surgical mask shows that there is definitely a decrease in covid prevalence, but, because of the necessary differences in standard error for the smaller sample sizes for each group individually, the confidence intervals for cloth vs. surgical individually are wider, overlap, and are not even definitively proven to be effective, with only the surgical mask being significant at the 10% level. Even with the large number of villages recruited into the study, the overall prevalence rates were low enough so as to not definitively establish the desired conclusions. Given the uncertainties in the study in general, you’d really like to see some slam-dunk numbers here.
Second, a substack site “bad cattitude” levies a number of criticisms. Some of them are, I think, too nit-picky, for example, leaning very heavily into complaints that the authors did not definitively establish that the villages were truly sufficiently identical to each other for the randomization to be effective. In particular, they did not have a starting value for covid-prevalence, just the ending point. It seems unlikely to me that there would have been such a difference as to have invalidated the study but he says “this is a tiny signal (7 in 10,000) [so] we need a very high precision in start state” and “even miniscule variance in prior exposure would swamp this.” It would be helpful to have seen some math demonstrating the possible effect of different levels of variance that are within statistical possibility.
This author’s larger criticism is of the self-reported nature of symptoms that I observed earlier. Now, we already know that there are two elements of Bangladeshi village culture that are “non-WEIRD” — the fact that mask color has a statistically-significant effect on whether villagers choose to wear them, and that mask-reminders have a dramatic impact on use. (Just try to imagine that happening in small town USA!) The substack author also points out that there was a very wide discrepancy between self-reports of mask-wearing (80%) in their own prior survey and actual use. It seems to me likely that Westerners cannot necessarily predict how Bangladeshi villagers would respond to being given masks, then being called and asked to self-report whether they have any of a set of symptoms, but it also seems to me that there’s a good chance that their response would not be the same as Americans, in one direction or another. That site also quotes twitter account @Emily_Burns_V, who says, “Is it possible that highly moralistic framing and monetary incentives given to village elders for compliance might dissuade a person from reporting symptoms representing individual and collective moral failure — one that could cost the village money? Maybe?” And, indeed, the study’s authors say that there was no effect of the text-nagging or the incentives, on mask-wearing, but do not report whether there are differences between these groups, and the symptom-reporting.
Finally, Bad Cattitude has an interpretation of the age-differences which seems more plausible than “masking had a greater effect on the old”: “the odds on bet here is that old people were more inclined to please the researchers than young people and that they failed to report symptoms as a result.”
One last set of comments on the study, from researcher Lyman Stone, again via twitter. He defends the study authors against the accusation that they failed to pre-test to establish a baseline, by saying that the study authors themselves acknowledged that this was still underway, and this was, after all, a working paper, not the final product, and reports that it is the norm to provide preliminary reports even when the data analysis is complete.
Stone also observes that the differences in results between cloth and surgical masks is an indicator that there was a sort of unplanned “blindness” to the study, in that both the cloth and surgical mask recipients were aware they were a part of a study, so if the effects we see are a result of their response to this, we’d see the same effects for both cloth and surgical — but we don’t. (Of course, Stats with Cats observes that the difference between the two groups is not a slam dunk because of confidence intervals, and, as tempting as it may be to do otherwise, it is important to take the confidence intervals seriously.) (For what it’s worth, Bad Cattitude rebuts the rebuttal in a follow-up piece.)
The bottom line: when this study first came across my twitter feed, I enthusiastically retweeted it. Now I’m disappointed — I would have really liked to have seen more answers, and be left with fewer questions that mean it becomes “one data point among many” rather than the slam-dunk evidence that some of its promoters think it is, especially since the whole debate has now resulted in mask-promoters asserting that mask-wearing is always and everywhere cost-free while ignoring that for some people it creates real health issues and for children, poses risks of developmental delay.
Finally, as a reminder for those who don’t know my background, very early in the pandemic I was not merely an enthusiastic mask-wearer, but a die-hard mask-maker, donating some 150 of them to healthcare workers and others, which means that anyone who judges these comments as those of a crazy anti-masker wholly misunderstands them.
Yesterday, the state of Illinois announced that suburban Cook County is now subject to covid mitigations, in which, as of tomorrow, indoor dining and bar service will be prohibited and groups at any one gathering will be capped at 25 people. As the Chicago Tribune reported,
By Wednesday, more than half of Illinois residents will be living under stricter measures meant to slow the latest surge of the coronavirus as suburban Cook County and the Metro East region outside St. Louis join four other regions where the state has shut down indoor dining and bar service and lowered the cap on crowds to 25.
A week ago, only one of the 11 regions in Gov. J.B. Pritzker’s reopening plan was subject to those rules. . . .
Suburban Cook County has had eight consecutive days of test positivity rate increases and seven days of increased hospital admissions. It is the first region to surpass the state-set thresholds for those two metrics at the same time. The other region have triggered tougher rules by reaching an 8% positivity rate threshold for three consecutive days. As of Friday, the rolling seven-day positivity rate for the Cook County suburbs was 7.7%.
With that context, I wanted to write down some of my recent thoughts on developments.
First, why did contact tracing fail?
Contact tracing was, after all, the subject of my May 15 Tribune commentary, in which I observed that the state’s reopening metrics required that for Phase 3, contact tracing would be fully-rolled out, and for Phase 4, contact tracing would be fully scaled up, so that tracing would begin within 24 hours for 90% of new diagnoses in a region. Turns out, Phase 3 began according to the timeline for all the other metrics, at the end of May, and Phase 4 began at the end of June. But according to the organization TestAndTrace, as reported at Patch, Illinois has a failing grade in their assessment of Illinois’ contact tracing, due to their very low number of tracers and lack of transparency about their progress.
With respect to Cook County, the Cook County Department of Health announced on June 11 the receipt of a $41 million grant to scale up contact tracing. But even just last week, Daily Line reporter Alex Nitkin had this to say:
Meanwhile, Cook County public health chief Dr. Kiran Joshi tells commissioners the county/city's joint contact tracing effort is deep in the recruiting process and expects "offers to go out in the next week or so."
Now, the question above is, I admit, partly rhetorical. I have my own suppositions as to why, when it really would have made a difference in the late spring/early summer, when cases were down and when Illinoisans were relatively more hunkered down — that is, when a contact tracing effort would have uncovered fewer contacts for any given individual — the state, and Cook County and the city of Chicago as well, fumbled this: the desire to create union jobs, for one, and the focus on “equity” even when a focus on “low-hanging fruit” might have been more effective. Various reports in the meantime have described the suspicion with which immigrants and low-income Chicagoans treat contact tracer outreach; focusing resources on parts of the state which would have a greater success rate, as well as more rural areas where there would have been fewer contacts to trace in the first place, would surely have found more success.
In any event, at this point, it is far less effective to contact-trace when cases are becoming increasingly prevalent, as is the case now.
And, in addition, it would appear that the state is misinterpreting the data that it does garner from contact tracing, in any case.
Earlier in the month, Capitol Fax provided a graph produced by the state which was used as justification for its focus on bars and restaurants. The graph is appallingly difficult to read (and is shown only as a picture, with no data accessible), but claims that, statewide, when contact tracees were asked where they had “visited or worked” within the past 14 days, the second-largest category of response was “restaurant/bar,” with 2300 responses. The top response was “other,” which includes “vacations, family gatherings, weddings, college parties.”
But this graph is exceedingly unhelpful. Respondents could give multiple answers, and the graph’s “n” is given as 17,939, but that’s the total number of boxes checked; a true “n” from such a survey would be the number of people surveyed. We don’t know what percent of tracees visited bars or restaurants, and, more importantly, we don’t know whether people who went to bars/restaurants were disproportionately likely to have been diagnosed with covid. In other words, to tell us something meaningful, this graph would need to be paired with another one, in which a random sampling of people who matched the demographic characteristics of covid-diagnosed tracing respondents.
And, in fact, here’s my transcript of Dr. Ngozi Ezike’s comments at the press briefing last Friday, upon being asked why bars and restaurants are being singled out for closure despite being linked to only 6% of outbreaks (about the 28 minute mark):
Ezike: An outbreak would be something if somebody works like say at a manufacturing plant and a lot of people work in close proximity and 50 people develop covid in that setting we would have that as a documented outbreak where this person knows that I was working next to this person, this person contracted the virus, a week later so did I, a week later this person did, three days later, so that is like a clearly documented outbreak. In most cases of covid, the person who has it cannot tell you exactly who they got it from, they cannot say, “oh, I was working in this setting and all these people got it and I got similar symptoms, so in the absence of a documented outbreak all those individuals that did contract the virus the way that you look at where they may have gotten it from is to look at the time at which, the time frame from when you catch the virus to when you show symptoms or to whey you’re diagnosed, in those preceding two weeks, we ask the cases, where have you been, and all of those places that they list, that they have been in the preceding two weeks are exposure sites. Any of those places could have been where they contracted the virus. And time after time, bars and restaurants come up as the number two or the number three place of all of these places frequented, so that’s why we put it as a high because it consistently comes up as a place where people who are infected listed as one of their exposure sites.
What’s remarkable is that Pritzker appears to recognized that this is a poor rationale for closing bars and restaurants, and he jumps in:
Pritzker: And I would just add that there are literally a dozen studies, many many articles about these bars and restaurants being exposure sites, and the effect of bars and restaurants on the spread of the virus and that is why there is a focus on bars and restaurants.
Ezike’s specialty is pediatrics and her expertise within public health comes from working on health care within juvenile detention centers. Is it possible that she just doesn’t have the grounding in statistics that’s necessary to grasp these concepts?
Second, why are hospitalizations level in suburban Cook County?
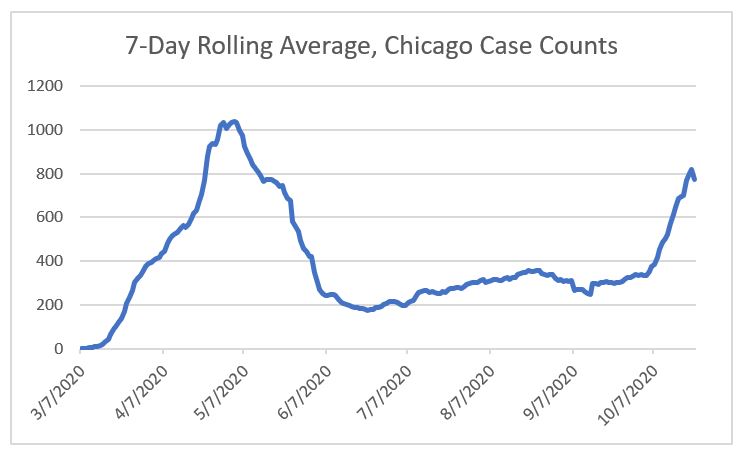
Wirepoints has been tracking key covid data for Illinois as a whole since early on. When cases rose starting in July, in a way that did not appear to be clearly linked to the ramping up of testing (because at that point the state had already increased testing substantially), I followed their tracking of hospitalizations and deaths and observed that these numbers were holding steady, in a manner that fit the theory that the rise in cases were due to increasing numbers of low-risk young adults becoming diagnosed, or that masks were having the effect of reducing the viral load and thus the severity of the infection.
But that’s no longer the case. On September 19, hospitalizations stood at 1,417. They rose gradually, to reach 1,575 on Oct. 3; since then they’ve risen steadily, to 2,605 on October 24.
What’s more, deaths have been increasing during the same time period. Ranging from the upper teens to the low 20s all summer and early fall, the 7 day average stood at 42 on Oct. 26. It’s also difficult to make a visual judgement, but there is no apparent lag, as you’d expect there should be, from the start of the increase in hospitalizations to the start of the increase in deaths; these are occurring simultaneously.
Frustratingly, it is not easy, from the information available at the Illinois Department of Health’s website, to look at hospitalizations by region or county. With a little bit of patience, we can look at admissions for Covid-like illnesses region-by-region:
Region 1, northwest Illinois: hospitalizations level over the summer, then steadily increase from 4 on September 20 to 14 on October 21.
Region 2, north-central-west: steady increase in hospitalizations over July (4 on July 3) to early August (12 on August 4), then another small increase in recent weeks (14 on Oct 22).
Region 3, central-west: again, small incease in mid-July, level to mid-October, then increase from 8 on Oct. 12 to 12 on Oct. 18.
Region 4, south- west (St. Louis area): relative peaks in late July and again in late August; decline since then to match the level of June.
Region 5, south: level/very gradual increase through September; then increase from 4 on Oct. 1 to 8 on Oct. 21.
Region 6, east: same pattern as south, very gradual increase through end of September, then jump: 8 on Oct. 2 to 19 on Oct. 22.
Region 7, far southern suburbs/exurbs: lots of bouncing around: peak in mid-August, decline, then increase from the beginning of October to now (6 to 16).
Region 8, western/far western suburbs: increase in mid-June, level through the end of September, then steep increase since then: 14 on Oct. 5 to 27 on Oct. 23.
Region 9, northeast Illinois (Lake and McHenry counties/far north suburban Chicago): increase in June, level through August, drop through mid-Sept. and level to the end of September, then increasing from 7 on Oct. 5, to 13 on Oct. 23.
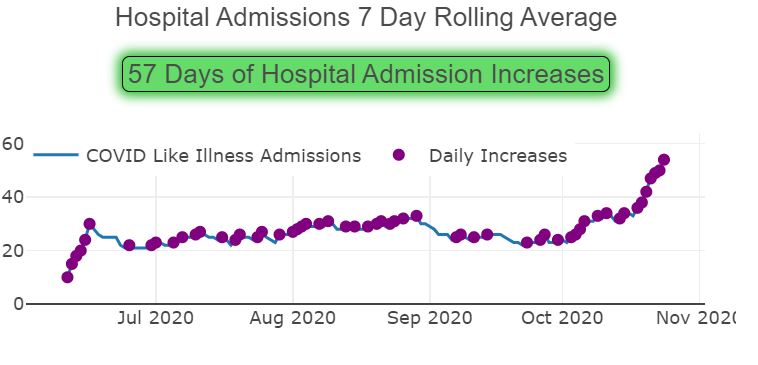
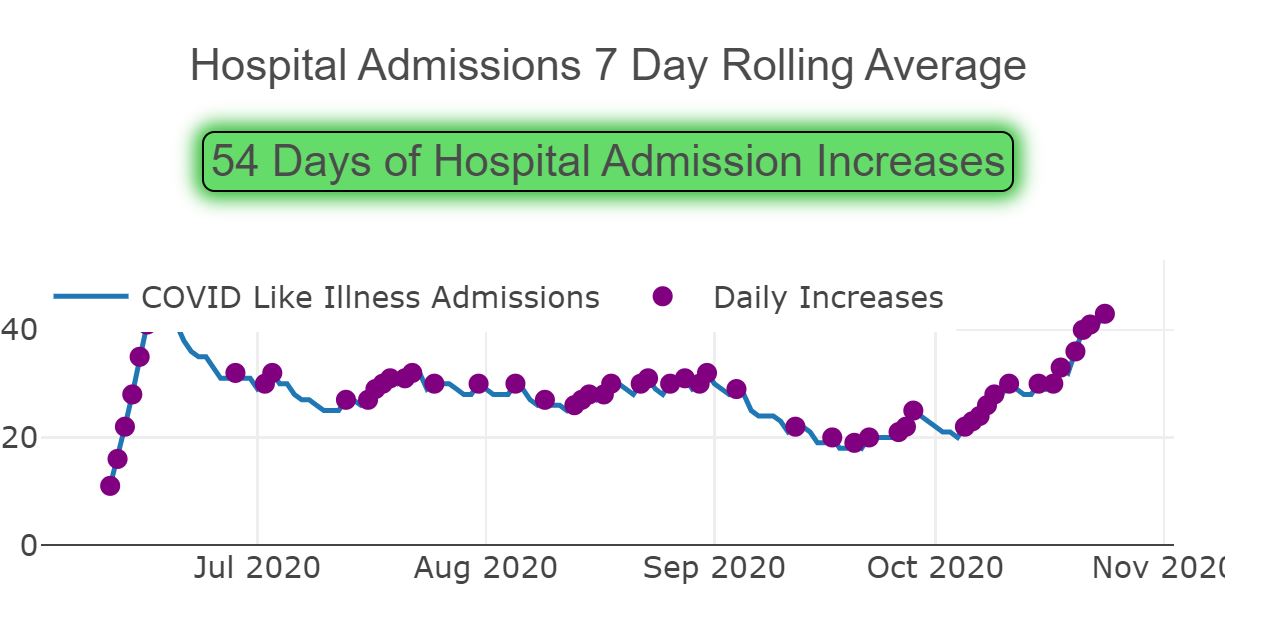
Region 10, suburban Cook County: level-ish through the end of August, a small drop through the end of September, then a jump from Oct. 2, at 23 to Oct, 22, at 49.
and Region 11, Chicago: level through July and August, drop in September to a low of 21 on Oct. 3, then up to 41 on Oct. 23.
(Note that the Wirepoints numbers are total hospitalizations; these are admissions on any given day.)
But, again, here’s suburban Cook County according to the IDPH dashboard:
Covid-like admissions, October 27 data. https://www.dph.illinois.gov/regionmetrics?regionID=10.
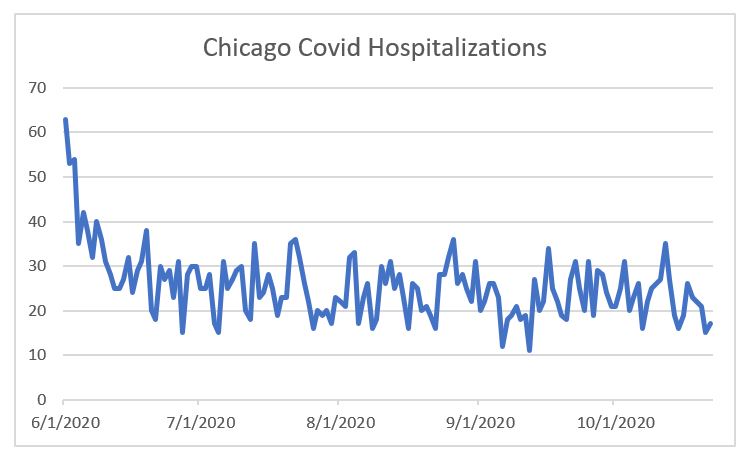
But at the same time, the Cook County Department of Public Health‘s own website’s reported hospitalizations have been level, showing no change other than a drop-off for the past week due presumably to lags in data reporting. (Note: as of today, they have removed the data on hospitalizations; I have requested an explanation.)
What’s going on? You’ll have to trust me that the CCDPH data was level, because it’s been removed, but is the fact that the state includes “covid-like illnesses” regardless of whether a patient has covid, causing an increase in the numbers? I can well understand using this broader definition back when testing was difficult, but covid tests are no routine for anyone who enters a hospital even for unrelated reasons.
Again, are hospitalizations due to covid really on the uptick? Or is it due to “covid-like illnesses”? Or — benefit of the doubt here — is there something faulty about the “covid hospitalizations” figure even after tests have become available without practical limits in terms of hospital access?
Third, what about Europe?
Biden, and Trump opponents generally speaking, are willing to say that a considerable number of America’s covid infections and deaths can be blamed on Trump’s poor management of the pandemic, and it’s easy to point to countries which have had extremely low infection rates — Japan, Taiwan, South Korea. It’s also easy to point to stunningly foolish things Trump has done and said, and the whole mask debacle, well, it’s been a debacle — insisting in March that masks were useless only to later on conclude they weren’t, but stoking substantial suspicion due to that prior insistence.
But claims that the US has been singularly incompetent in managing the pandemic are falling apart.
According to the Financial Times‘ website, measured on a cases-per-million basis, averaged over 7 days, the European Union’s rate equaled that of the US on October 11 or thereabouts. Now it’s rate is substantially higher, at 284.2 cases per million, compared to 200.7 in the US (as of Oct. 22 and 23, respectively). In fact, very few countries within Europe are lower than the US, and many of those which are, are seeing steady increases. Even Germany, lauded for its successful handling of the pandemic early on, is now seeing a surge in cases, with a 14 day change of 191% for new cases and 198% for deaths, compared to an increase of 40% and 14% for cases and deaths, respectively, for the US, according to the New York Times. (Remember, to increase by 191% is not to double, but to triple, that is, for the new case rate to be 3 times that of the original rate.) That means that seems quite likely indeed for Germany to reach our level of cases relative to the population by Election Day, which would be ironic when Joe Biden claims that he would have had German-levels of success in avoiding infections in the U.S.
Why are cases spiking in Europe?
Does that mean that there’s nothing, really, that can be done but hope that a vaccine and/or an antibody treatment is approved, manufactured, and distributed? What does an observation of the case increases in Europe mean for our decision-making about whether to shut down restaurants or merely restrict their capacity, or even to re-institute lockdowns?
This is where I end, as I don’t have answers to these questions, and I’ve achieved my short-term goal of writing now new information I’ve learned and issues I wanted to share.
It’s right there in black and white: contact tracing is a key part of Illinois Gov. JB Pritzker’s “Restore Illinois” plan. To move from Phase 2 to Phase 3, permitting the opening of child care, retail, and gatherings of 10 or fewer people, requires the beginnings of “contact tracing and monitoring within 24 hours of diagnosis.” To move from Phase 3 to Phase 4, permitting the opening of restaurants, personal care services, health clubs, and schools, as well as gatherings of 50 or fewer people, requires fully scaled-up contract tracing, that is, “for more than 90% of cases in region.”
But as I wrote last Saturday at the Chicago Tribune, however crucial contact tracing is, the state has provided virtually no information on its timing or its progress in implementing the program.
Only just today did the Department of Public Health provide a press release on the topic (can I take credit for this?), informing residents that county public health departments will actually be running the initiative, with funding and technical support from the state, and with Partners in Health in an advisory role. Two specific counties will be “immediately” piloting the program. The governor further stated at today’s (Monday’s) press briefing that at present 29% of diagnoses are “engaged in a tracing process” and “that’s a number we want to push as high as possible, to the industry standard of over 60%.”
Despite this, last week Pritzker announced that “all regions across the state are now on track to meet the metrics needed to move into the next phase of reopening.”
How does this make sense? With only 11 days until the first possible “Phase 3” date, and with only a 2-county pilot program in place, how can the state be on track to meet its Phase 3 contact tracing requirement?
And how does a verbal target of aiming for “the industry standard of 60%” match up with the Phase 4 requirement of 90%?
What’s more, the state provides regular updates to metrics in the areas of testing and hospital admissions and resources, but no updates on contact tracing.
It’s as if they’ve forgotten about these requirements.
Has the state abandoned them, that is, continuing to strive for additional capacity but no longer requiring implementation/scaling to move to the next phase?
And, if so, why is the state not revising its plan, but instead simply treating them as if they don’t exist?
My guess: the governor knows there is tremendous pressure to revise other components of the plan: the inclusion of very geographically distinct counties adjacent to “collar counties” in the same region as Chicago, the continued closure of restaurants until Phase 4, the limitation on gatherings to 50 persons regardless of the capacity of a given facility, and so on. Were he to revise the contact tracing component, he would further increase calls for revisions of other sorts. So long as no one with any particularly strong voice or much political power calls him on this, he continues to be enabled to insist that his plan is unchangeable, set in stone, rather than risking opening it up to the sort of negotiation which he insists is impossible because he is guided solely by “science” and “data”.
Now, this is an admittedly cynical answer, but I can’t make sense of this any other way. And, much as I hate for it to be true, as it implicates a wide range of bureaucrats as well in this convenient omission, it does, at the same time, offer some firmer reason to believe that, however painfully delayed Phases 3 and 4 are implemented, however many restaurants and other small business will shut down, it will at least not be delayed even further.
Millennium Park, Chicago, via Pixabay, https://pixabay.com/photos/concert-park-venue-music-artist-4634009/, public domain
Readers on other platforms will know that I have been sewing facemasks. My current count is 120 given away; I have a further 20 that are waiting for homes, plus, of course, the ones for our family. I’d been saying, “it makes me feel useful,” especially knowing that my writing at Forbes on retirement isn’t catching many eyes when it’s a stretch to tie things to the pandemic. But I realize that I had been treating it as something of a magical act: if I sew face masks, then things will work out OK.
In the meantime, the CDC’s initial insistence that face masks had no use, and failure to explain themselves sufficiently since then, has now resulted in far too many people rejecting face masks (“the CDC said there’s no point, so clearly the requirement now is just government overreach”). And at the same time, when I go to the store, I see lots of people with manufactured disposable face masks of the sort that we’re told are “reserved for healthcare workers.” The city is sponsoring giveaways — again of disposable masks; another group has sourced fabric masks out of Vietnam. It all leads me to question the utility of the masks I’ve been sewing.
Separately, the other day, in response to a lawsuit, Pritzker added “gathering for religious observance in groups of less than 10” to the list of permitted activities in the state of Illinois. And the neighboring diocese, in fact, permits coming to church for silent prayer; in the Archdiocese of Chicago, everything is shut down tightly, with no indicator that this will change, only a vaguely-worded statement that the archdiocese is “engaged in planning” on the matter.
And now Pritzker has released his “Restore Illinois” plan. I’m not happy. More specifically, it’s so discouraging I feel as if I’ve wasted my time battling the broken threads and birds’ nests of my 60s-era sewing machine, that only a move out-of-state would actually solve anything.
On the one hand, the plan is to be based on regional benchmarks. That’s a plus, I suppose, but my suburban town is lumped in with the city, so it doesn’t help me.
Here are the phases:
Right now, we are in “Phase 2” — a retroactive description of the governor’s changes to his stay-at-home order, with small loosenings of restrictions (curbside pickup rather than complete closure for non-essential stores).
Phase 3 would permit the reopening of “non-essential” businesses and manufacturing; retailers may open with capacity limits; barbershops/salons may open with restrictions; health and fitness clubs can provide outdoor classes. Healthcare providers may also re-open. Heavy, heavy restrictions remain including no gatherings of more than 10, no schools. “Limited child care and summer programs open with IDPH approved safety guidance” — and no further explanation about what this might mean. (Currently there are daycares open for essential workers — would these need-based restrictions remain? Or would the requirements be so stringent that it would effectively result in providers declaring they can’t meet them?) Some elements that I had hoped would be a part of a next-phase, such as outdoor dining, are not here. And a limit of 10 persons is unnecessarily restrictive in cases such as, for example, religious services in buildings large enough to accommodate more than that with wide spacing between individuals or family groups.
In order to declare Illinois (or a region thereof) in Phase 3, the state will require:
Less than a 20% positivity rate (that is, percent of tests which are positive),
No increases in admissions for 28 days,
Available capacity of 14% of ICU beds, hospital beds generally, and ventilators,
Testing widely available,
and the implementation of contact tracing procedures (I think – that’s how I interpret “begin contact tracing and monitoring within 24 hours of diagnosis”).
The measurement starts as of May 1, so that the earliest a region can be declared in Phase 3 is May 29, even though, for all but the Northeast (Chicagoland) region, the benchmarks could well be met sooner but for that seemingly-arbitrary requirement, according to a tracking document which the state, it seems, intends to update regularly. And how long would Phase 3 last? The two additional requirements to move to Phase 4 are for testing to be available to all, regardless of risk factors or symptoms, and “begin contact tracing and monitoring within 24 hours of diagnosis for more than 90% of cases in region” — which I why I’m understanding the Phase 3 requirement to be more about contact tracing being underway.
But what would the timeline look like for contact tracing? According to The Southern, the initiative “likely won’t begin in earnest until sometime in late May.” How long would it take to reach this 90% benchmark? I’m not finding anything further on timing in the scanty reports on the initiative, not even speculation of how long it could last, but knowing bureaucracy, this seems a monumental hurdle. (Massachusett’s program is referred to as a model; their program has been running for a month and includes 17,000 people, including infected people and their contacts, relative to 70,271 positive tests so far.) Even discarding my skepticism, how long do Pritzker and his advisors actually have in mind when they set this marker for the transition to Phase 4?
Phase 4 removes many restrictions but keeps many more. Schools are open, all outdoor recreation allowed, bars and restaurants are open, etc. However, crucially, there continue to be capacity limits on theaters, restaurants, and retail, and no gatherings of over 50 people are permitted.
And Phase 5? To permit gatherings of over 50 will require that
Either a vaccine is developed to prevent additional spread of COVID-19, a treatment option is readily available that ensures health care capacity is no longer a concern, or there are no new cases over a sustained period.
Separately, the document indicates that the last condition may be met through “herd immunity or other factors” and that the treatment must be “effective and widely available” so as to suggest that the demand goes well beyond the moderate effects of the new drugs or ventilator-avoiding methods thus far.
And this is where it all seems to lose touch with reality. We may never have a vaccine, certainly not for a year or even much longer; and the threshold for an “effective” treatment is undefined but we may not have something that meets these requirements.
The clarifications at today’s press conference (via Capitol Fax) don’t help, either. Pritzker seems to suggest that “treatment” is “a very successful treatment” or, separately, a “highly effective treatment.” Asked about schools having more than 50 students, he says,
There would be strict IDPH guidelines for schools and we talked about this early on when we were trying to figure out if we needed to close schools or not, that, could you have classrooms of [garbled] kids meeting, if the restriction was 50 for example. And would that work and so the answer is IDPH is going to be working with schools on how they can best do this coming into the fall assuming that we’re in phase four.
Does Pritzker actually have a plan? Has he given serious consideration to how his phases will actually work in the real world? It certainly doesn’t appear as if he has a real answer with respect to children (neither “the data shows the risk to children is virtually nonexistent” nor “we’ll ask schools to come up with as many precautions as possible and eliminate assemblies and other gatherings”). Is he relying on the emergence of a game-changing treatment over the summer?
And nowhere in this plan is a mention of nursing homes and assisted living communities. When will their residents be able to see their families again, or even gather within the community? For those with cognitive issues, this is not merely about being patient but about their well-being.
Democrats are praising the plan, again according to Capitol Fax, with Senate President Don Harmon calling it “forward-looking” and Comptroller Susan Mendoza, “carefully-thought-out” and “science-based.” But there are so many holes — and, no, there is no reference to any sort of footnoted, detailed second document.
The bottom line is that this document is a serious disappointment. Using labels such as “recovery,” “revitalization,” and “restored” is nothing more than a cruel joke as long as the plan is so vague and unrealistic.
Today marks the start of the mask-mandate in Illinois. All persons over age 2 must wear a face mask in any public place in which they cannot maintain a six-foot distance from others — that is, indoors while shopping and in any crowded outdoor place.
Tutorials exist all over the internet: Save the manufactured masks for healthcare workers; use fabric. Use tightly-woven cotton, if possible. Add a non-woven inner layer via an opening for a filter, or a third layer of flannel. The Illinois mandate does not specify that one must wear a “face mask” per se but a covering of the nose and mouth, so that improvised options such as a bandana are also acceptable.
The Chicago Tribune has reported on various mask giveaways such as the groupMasks4Chi which is importing fabric masks from Vietnam, as well as various community distribution efforts (which appear to be oriented around manufactured one-time masks). And, of course, large numbers of home sewers have been making masks and selling or giving them away — to nursing homes and assisted living communities, grocery store baggers, anyone they come across who’s in need. (Yes, I’m one of them — my current tally is 118 given away, and another dozen in various stages of completion — and it surprises me that the giveaway efforts don’t have a parallel organized effort to collect donations for the general public.)
Does Gov. Pritzker have the legal authority to mandate mask-wearing?
To be honest, I’m not sure. Downstate Rep. Darren Bailey filed suit against the stay-at-home order’s extension, and won a court victory, for himself, and subsequently Rep. John Cabello of Machesney Park filed suit calling for the same ruling to be applied to all Illinoisans. Are their legal arguments valid? I’ll be honest — I am not seeing reporting that answers that question. Instead, Pritzker and others react as if the pursuit of the greater good of public health prohibits even the asking of that question, though, at the same time, Pritzker has, in breaking news, rescinded a part of his executive order that prohibited religious gatherings, in reaction to a separate lawsuit. (Previously, even drive-in services were prohibited; now they will be allowed.)
And a Chicago Tribune editorial today called for the legislature to meet. Not only could they legislatively affirm Pritzker’s orders, but they could attend to other pressing state business, including the deadline on Monday for placing on the November ballot an amendment to end gerrymandering of General Assembly districts. The editorial notes that a one-time meeting would be sufficient for the legislature to enable virtual meetings; alternatively, Pritzker could use his power to convene the GA elsewhere — columnist John Kass suggests, for more-than-sufficient social distancing, the United Center. Of course, Kass also suggests that, behind the scenes, it’s House Speaker Michael Madigan calling the shots, and refusing to meet, so that Pritzker takes the heat.
What’s more, I’m seeing on Facebook plans to circumvent the mask requirement. After all, the ruling provides an exemption for those who cannot medically tolerate a mask. Claim to those who question you that you’re exempt for medical reasons, further insist that your medical privacy rights prohibit their questioning the specific ailment you have and, voila, you can skip the mask.
But here’s the bottom line: even if you object to the mandate, you should still wear a mask.
Yes, the CDC was foolish in its prior insistence that there is no value in mask-wearing, and, though I’ve speculated elsewhere as to why they did so, I’ve not seen a definitive (and convincing) explanation for this, nor for why, on April 3, they changed their recommendations. But even the Illinois Policy Institute, ordinarily an opponent of Pritzker, states plainly:
The point of wearing a mask is to protect others. The idea is that if one person is an asymptomatic carrier of COVID-19, wearing a mask will limit their ability to transmit the virus to others.
Folks, I’ve been sewing face masks since so early on that when I first picked up fabric and notions I was able to get not only elastic but also “fun” Marvel print cotton fabric straight off the store shelves. Perhaps I’ve spent enough years as an international retirement actuary to have had on my radar more than others that we can reasonably look at what’s going on in other places, and early on it was clear that places like Hong Kong and Taiwan had both a firmer control on the coronavirus than elsewhere and had a practice of wearing masks. (Yes, I first blogged about this on my personal blog on March 16, in which I speculated about whether face mask-wearing could ever take root in the U.S.; four days later, I had convinced myself that sewing was the right thing to do, even though the calls were mostly for healthcare workers. When did I first don a face mask myself when going out to the store? I’m not sure.)
It might feel that wearing a mask gives a “win” to Pritzker, that you’re sacrificing your freedom. I get that.
But face mask-wearing is important to protect those around you, in the event, however unlikely you consider it to be, that you have yourself been unknowingly infected. And even if you judge it impossible to have been infected, face mask-wearing is a visible way to encourage those around you to wear masks, so that any one of your friends, neighbors, or fellow shoppers who is unknowing infectious, will wear a face mask and protect those around them.
I suspect that those who protest this order nonetheless consider themselves to be good citizens who care about the welfare of others, even if they’d rather it not be mandated. I, too, wish we had all adopted mask-wearing practices without a mandate. But that’s where we are. And, to be honest, I am at least glad not to be the “weirdo in a mask” any longer.